
In an era of tightening state budgets, the two major spending areas have been health care and prisons. A new study shows the intersection of these two areas, prison healthcare, has grown more than 50 percent from 2001 to 2008. Per data collected from 44 states, health care expenses accounted for one-sixth of the $36.8 billion the states spent on prisons in 2008.
Inmates’ health, the public’s safety, and taxpayers’ total corrections bills are all affected by how states manage prison health care services. Effective treatment of inmates’ physical and mental ailments, including substance abuse, improves the well-being of prisoners and can reduce the likelihood that they will commit new crimes or violate probation once released.”
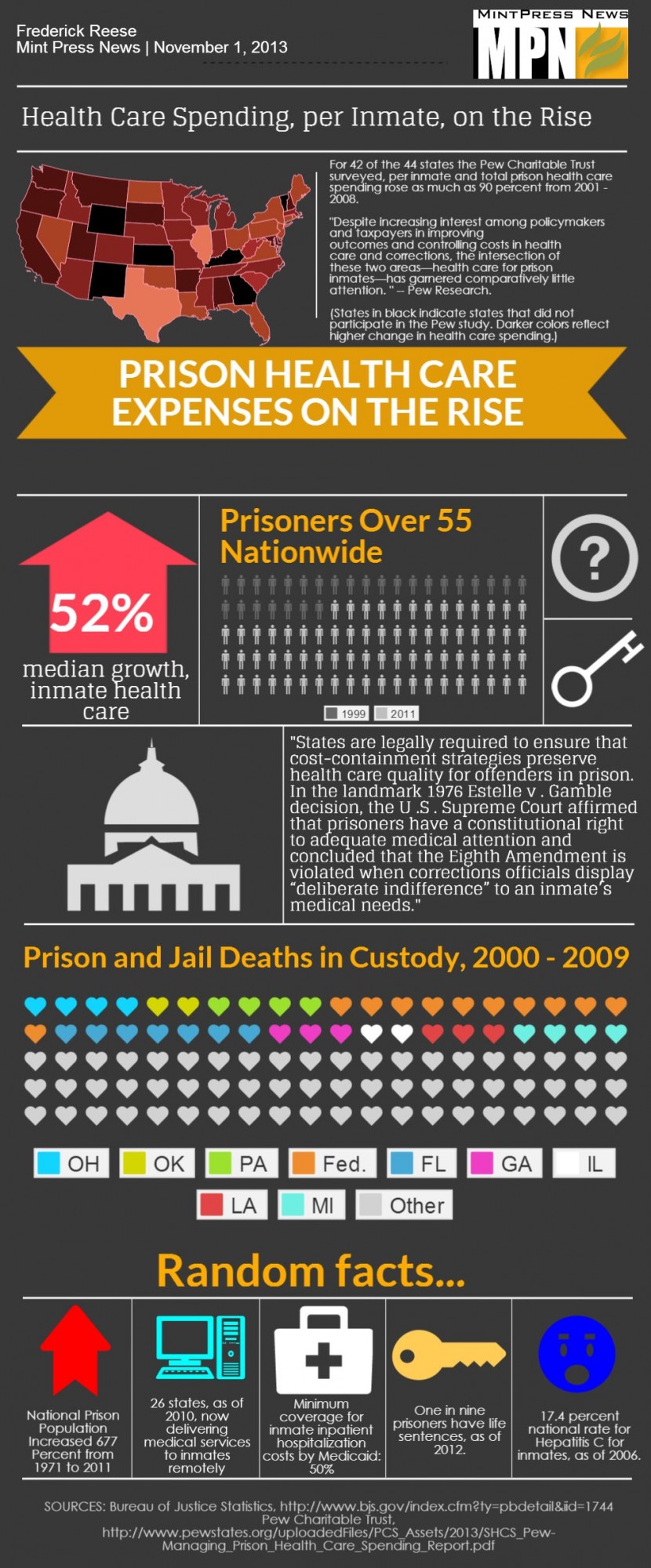
The study — conducted by the Pew Charitable Trust and the MacArthur Foundation — found that for 42 of the states, prison health expenditures grew over the seven years of the study, with a dozen states seeing 90 percent growth or more. Per-inmate health care spending rose an of average 32 percent, with growth in 35 states.
The survey gives primary credit for this growth towards the increase in the national prison population — which has increased 677 percent from 1971 to 2011; the U.S. prison population is estimated at 1,538,854 inmates — but also to an increasingly aging prison population, a prevalence of mental illnesses, infectious and chronic diseases among the population, and access difficulties to hospitals and care providers.
Prisons: ‘A unique opportunity’ for health care?
In 2009, Georgia paid $8,565 per year in health care per inmate aged 65 or older. The average cost per under-65 inmate in the Georgia system is $961 per year. Despite the cost, the prisons may be offering a service that would be otherwise unavailable for many of the inmates on the outside world.
“[It has been] suggested that correctional facilities may present ‘a unique opportunity’ to provide [inmates] with ‘at least some medical care that they haven’t gotten otherwise’,” wrote Amy Smith for a National Academy of Sciences report.
“Prisons are coming to function as a massive organ of delivery for public health for people who are involved in the criminal justice system. … [It has been] noted that jail provide a strategic public health opportunity to screen and diagnose infectious diseases among persons who often evade traditional healthcare systems and yet are at high risk for illnesses, such as HIV infection and viral hepatitis, and prisons provide an opportunity to diagnose and treat chronic diseases, such as diabetes, hypertension, addiction, and mental illness among persons who frequently have not sought or had access to treatment prior to incarceration.”
“On the other hand, the prison environment may have adverse effects on health … The nutritional value of meals is far from ideal, because energy-dense (high-fat, high-calorie) foods are still common in prison meals. Smoking also remains a serious problem, despite the trend toward smoke-free correctional facilities. Poor ventilation, overcrowding, and stress may exacerbate chronic health conditions. … Case studies have also revealed widespread and serious reactions to segregation units, in which inmates are restricted to isolation cells for 23 hours a day. The restriction of movement and deprivation of human contact triggers psychological responses, ranging from anxiety and panic to hallucination.”
Misusing Medicaid?
Some states have started using Medicaid to defer some costs of providing inmate health care. While Medicaid cannot be used to pay for in-prison health care, it can be used for out-of-prison care, such as surgery and rehabilitation. States that have accepted the Medicaid eligibility expansion under the Affordable Care Act have the potential of significantly lowering their prison health care bill.
“The relatively rare use of Medicaid to finance prison health care is due in part to state and federal policies governing the jointly funded program,” said the Pew-MacArthur report, “Which limit both the number of eligible inmates and the types of care covered.”
“These factors have restrained the potential savings states could realize through this strategy. Currently, federal law requires states to cover only certain populations, such as low-income children and low-income pregnant women, through their Medicaid programs. Inmates who fall into one of these categories are eligible for Medicaid, and if they are enrolled in the program, states can seek federal matching funds to pay for some health care services that these prisoners receive. Most inmates, though, are nondisabled adults without dependent children, a group generally not eligible for Medicaid.”
“In states that expand their Medicaid programs under the ACA in 2014, however, coverage will be available to low-income childless adults, making more prisoners eligible. These states also will receive an enhanced federal reimbursement rate for newly enrolled inmates’ care.”
For states that have participated in Medicaid reimbursements for inmates, the savings have been significant. Mississippi reports a savings of roughly $6 million per year, while Louisiana reported a savings of $2.6 million for 2009 and 2010. New York reported savings of $4.5 million as of December 2012. That state’s comptroller estimates a potential savings of $20 million per year, without factoring in any additional savings from the state’s acceptance of the Medicaid expansion.
Michigan is estimated to save nearly $250 million in inpatient hospital services during the first 10 years of implementing the state’s Medicaid reimbursement under the ACA expansion, according to the Center for Healthcare Research and Transformation at the University of Michigan. California is slated to save as much as $70 million per year.
Expert: Lack of care so bad it violates 8th amendment
Along with expanding parole programs like compassionate release — where non-threatening elderly or terminally-ill inmates are released when they can no longer take care of themselves in person — Medicaid can offer relief on prison health care spending with programs like video-conferencing between inmates and doctors and remote diagnosis systems.
Not everybody, however, support the use of Medicaid in this manner. “By definition, those state prisoners in state facilities are the obligation of the state and that obligation should not be transferred to the federal government … I think most people would come down on the side that Medicaid was never intended to pay for the medical care of people in state custody,” said Dennis Smith, former director of the Centers for Medicare and Medicaid Services under President George W. Bush. “It’s a very significant issue for the federal budget and Congress better close that loophole quickly.”
Despite the high levels of spending, large numbers of prisoners are critically in need of medical and psychiatric treatment. Per a 2009 study in the American Journal of Public Health, 14 percent of federal prisoners, 20 percent of state prisoners and 68.4 percent of local inmates have not seen a health care provider of any kind since incarceration, despite persistent health problems.
“There’s some alarming data that suggests that those [inmates] with chronic conditions don’t get the care they need when incarcerated, and that’s Eighth-Amendment illegal,” said Craig Blakely, co-author of the Pew-McArthur report and professor for health policy and management at Texas A&M University. “The whole war on drugs has made a disaster of our judicial system and created a nightmare we can’t control.”
“Given the huge cost of incarceration, we’re foolish not to ensure that inmates get the basic care that would allow them to have a better chance of rehabilitation. This suggests the need for universal access to health care.”
25 states and the District of Columbia are currently slated to expand Medicaid coverage.